My thoughts on Watt:
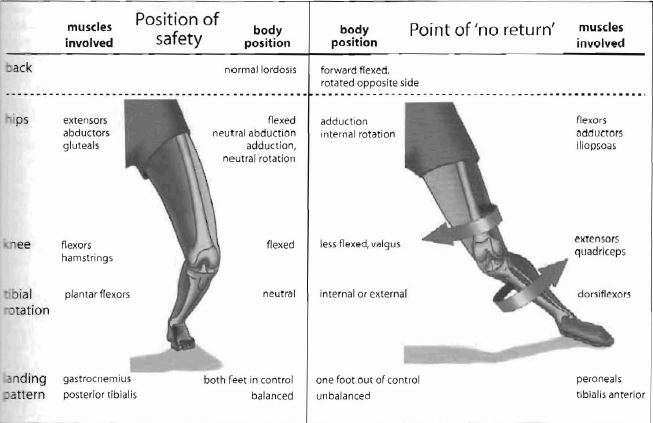
Unequal lower limb loads are often driven by dysfunction of the core/back. An extremely important factor of core stability is its ability to allow the player to control the pelvis on the hips and lower extremity in space via the stabilization functions of the abductors and rotators of the hip. Once the core/back becomes compromised.......... weakened/dysfunctional..........the knee stability is adversely affected with the knee becoming highly exposed to the risk of all injuries. With a tibial plateau fracture, in 30-40% there is an associated ACL or MCL tear, as well as meniscus damage.
A DIAGRAGM THAT I HAVE POSTED PREVIOUSLY:
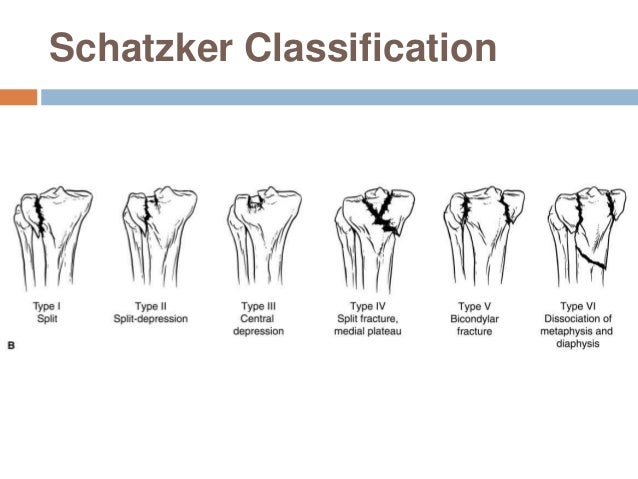
I don't know that the Texans will reveal the entirety of the injuries. But if it is a significant class of plateau injury, which at this point in time, I would say that it is, especially since it is all be a given that it will require surgical hardware reconstruction........that would mean that Watt is through for the season if not for longer. Even if it is a non-displace fracture that is treated without surgery, we will not see him this season.
Keep in mind that as the fractures traverse the cartilage surfaces, loss of overlying and directly adjacent articular cartilage is inevitable.


")