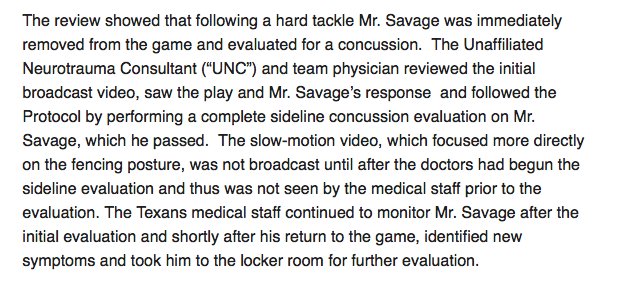
Savage has finally been placed on IR.
It's way too late in coming.......and should have been based on common sense from the very beginning. In response to the ridiculous decisions made with Savage (and also Russell), the Concussion Protocol has been altered.
The important changes:
• A central UNC will be stationed in the NFL's command center to assist in broadcast oversight at each game;
• Any sign of impact seizure will be considered the same as loss of consciousness, and the player will be out for the game;
• A referee who removes a player from the game for suspected head trauma must notify the medical staff;
• A player who exhibits gross motor instability or significant loss of balance must be taken to the locker room for evaluation if it is not diagnosed as an orthopedic injury;
• A player who is evaluated for a concussion must be re-evaluated within 24 hours, even if the player has an off day;
• A third UNC will be on site for the playoffs and the Super Bowl, in addition to the two already assigned to each regular-season game.
LINK








 Longhorn NetworkVerified account@LonghornNetwork
Longhorn NetworkVerified account@LonghornNetwork