CloakNNNdagger
Hall of Fame
So much to respond to, first I and most here don't disrespect JD & as you identify he's very good. His cap hit if tagged twice is close to $35-38 million so 20 million avg for first 2 years isn't that crazy and I think Gains would do that. Problem is of course Clowney wants more GTD and where talks break down. The knee doesn't get better sitting out. It's all risk and gamble for both sides. A player of his skill and productivity should sign an $80 million 4 year deal with say $20 GTD knowing second year will be GTD game one. He could sit out all off seasons and play sparingly some in preseason. He doesn't need practise to play well. Last two years could have incentives easy to reach + per game bonus of one million per. If used up after 2 seasons no one will offer much. Team will be good with JD but could be much better with what we get in trade now. If he's about money. I'm cool with it. Go to Gaines say" loved time here but need more than you want to pay. Get as close to this number for me and best deal for you and I sign tender and hope see you in Super Bowl."
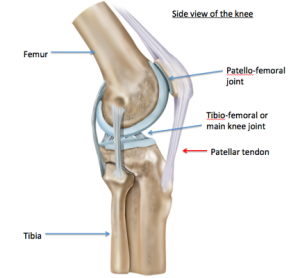
In order to try to better understand the Texans' reluctance to give Clowney a long-term contract with high guaranteed monies, it's important to understand the natural history of patients having undergone microfracture surgery on the knees............While reading this, keep in mind that in December Clowney will be 5 years post his microfracture procedure.
Despite the popularity, there is increasing evidence that also questions the value of microfracture in knees. Recent orthopedic reviews report that the long-term clinical results of microfracture are no better than those for patients who do not have microfracture, and that microfracture is not without risks
Orthopedists Goyal et al. reviewed all Level I and Level II studies (these are studies with the greatest confirmed validity) in the world medical literature and concluded that in the short-term, for young patients with small lesion sizes and low post-operative demands, microfracture was associated with good clinical outcomes. However ‘ beyond 5 years post-operatively, treatment failure after microfracture could be expected regardless of lesion size ’.
Another study has highlighted the risks associated with microfracture; that disruption of the subchondral plate (a support layer) upon drilling into the marrow predisposes the bone to the development of subchondral cysts and fragile or brittle bone, subsequently accelerating osteoarthritis.

Last edited:





 . Hoping just a rock in his shoe
. Hoping just a rock in his shoe 
